INFORMATION AVAILABLE IN ENGLISH, GUJARATI AND HINDI
Pleural Effusion (Empyema) is a condition where pus collects in the pleural space (space outside the lung and inside the chest wall, often as a complication of pneumonia.
The lungs and inside of the chest cavity have a smooth covering called the pleura that lets the lungs expand without rubbing on the inside of the chest. The two layers of pleura are usually in close contact with only a small space in between (pleural space) filled with a small amount of pleural fluid acting as lubrication.
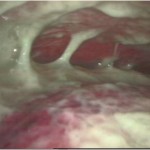
This complication of pneumonia usually occurs in three stages. Initially, clear fluid collects up in the pleural space which can then become infected. The fluid thickens and can affect the pleura, causing sections to ‘stick together’ eventually forming ’pockets’– this is called empyema. The infected fluid stops the lungs inflating completely, causing increasing breathing difficulties.
What causes empyema?
Empyema usually develops following pneumonia – various bacteria can cause pneumonia (most common ones are Staphylococcus pneumoniae and Staphylococcus aureus). Empyema seems to becoming more common, particularly in young children aged one to four years. It tends to occur during winter and spring season, when pneumonia and other chest infections are more common. Sometimes tuberculosis may also be a cause of empyema.
What are the signs and symptoms of empyema?
Empyema is usually suspected when a severe bout of pneumonia does not improve with treatment. Children usually show symptoms of being generally unwell with a high temperature. They may find breathing harder than normal, struggling to catch a breath. Their heart rate may also be higher than usual. Some children may describe pain in their chest when breathing.
How is empyema diagnosed?
If empyema is suspected, a chest x-ray may be the first test suggested to confirm or rule out the diagnosis. Chest x-rays will show white areas that suggest fluid. An ultrasound of the chest is more precise at showing the amount of fluid and the exact location and whether there are any pockets. In some cases, the doctor may also ask for a CT Scan of the chest to make sure that the child does not have any structural problems with the lung like a lung abscess which may have caused an empyema.
How is empyema treated?
Empyema previously used to be treated by placing a chest drain in the chest and with intravenous antibiotics as well as medicines to stop the pus clumping together.
However, nowadays with the advance of minimally invasive surgery, Empyema is treated with VATS (Video assisted thoracoscopic surgery) wherein a telescope is inserted into the chest cavity and all the pus is removed under vision. The pus pockets are broken down and washed with antiseptic liquids and a chest drain is placed. The surgery is completed with 2 or 3 5 mm instruments rather than placing a big cut on the chest. Also as the procedure is done undervision, the doctor is sure that the pus has been completely cleared and the child also recovers early.
What happens next?
The outlook for children with empyema is usually good once it has been diagnosed and treated promptly. Long term lung damage is rare. With thoracoscopy, the recovery is just in a few days. Once the lung is completely expanded as seen on follow up x-ray, the chest tube is removed and the child is sent home on oral medications. They will also need regular follow up clinic appointments, usually involving a chest x-ray, to check that the pleura is healing properly without any problems.
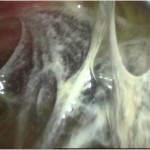
 Early Stage of Empyema (At Thoracoscopy)
Early Stage of Empyema (At Thoracoscopy)

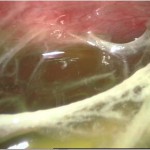
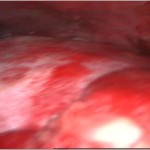
 Late Stage of Empyema (At Thoracoscopy)
Late Stage of Empyema (At Thoracoscopy)
 Lungs seen after clearance of Empyema (At Thorascopy)
Lungs seen after clearance of Empyema (At Thorascopy)
 Late Stage Empyema (Needing open surgery)
Late Stage Empyema (Needing open surgery)
GUJARATI
એમપાઈમા
એમપાઇમા ન્યુમોનિયાને કારણે ફેફસાંની બહારના ભાગમાં થતાં પાણી અને પરૂના ભરાવાને કહેવામાં આવે છે. સામાન્ય રીતે ન્યુમોનિયા દવાઓથી સારું થઈ જાય છે પરંતુ બાળકમાં જ્યારે રોગ પ્રતીકારક શક્તિ ઓછી હોય અથવા જંતુઓનો પ્રભાવ વધારે હોય તો ન્યુમોનિયાના એક કામ્પ્લીકેશન તરીકે છાતીમાં ફેફસાંના બહારના ભાગમાં પરૂ અને પાણીનો ભરાવો થાય છે જેને એમપાઇમા કહેવામાં આવે છે. એમપાઇમામાં ફેફસું દબાણમાં આવે જેથી બાળકને શ્વાસ લેવામાં તકલીફ પડે છે અને તાવ પણ ખૂબ જ આવે. પહેલા એમપાઇમાની સારવાર માટે બે પાંસળીઓ વચ્ચે નળી મૂકી પરૂ આપોઆપ બહાર નીકળે અને સુકાય તેની રાહ જાવી પડતી હતી. આ માટે બાળકને ઘણીવાર અઠવાડિયાઓ અને મહિનાઓ સુધી હોસ્પિટલ માં રહેવું પડતું. હવે આધુનિક સાધનો અને લેપ્રોસ્કોપીના આગમન પછી બે પાંસળી વચ્ચે દુરબીન મૂકીને ફેફસાંની બહાર આવેલું બધૂજ પરૂ અને પ્રવાહી સંપૂર્ણપણે સાફ કરવામાં આવે છે. ફેફસું સામાન્ય રીતે ફૂલી જાય તેની ચોકસાઈ કરીને આૅપરેશન થઈ શકે છે. આ આૅપરેશન પછી બાળકને ત્રણ થી પાંચ દિવસ હોસ્પિટલ માં રહેવું પડે છે અને બાળક સંપૂર્ણપણે સ્વસ્થ અને સારુ થઈ જાય છે. આ દુરબીનની ટેક્નીકને થોરેકોસ્કોપી કહે છે. •
HINDI
एमपाइमा (छाती में रसी)
न्युमोनिया के कारण फेफड़ों के बाहरी भाग में उत्पन्न होने वाले पानी और रसी के जमाव को एमपाइमा कहते हैं। सामान्यतः न्युमोनीया दवाइयों से ठीक हो जाता है। लेकिन बच्चे की रोग प्रतिकारक शक्ति कमजोर हो अथवा किटाणुओं का प्रभाव अधिक हो, तो न्युमोनिया की जटीलता के कारण छाती के भीतर फेफड़ों के बाहरी भाग में पानी और मवाद का जमाव हो जाता है, जिसे एमपाइमा कहा जाता है। एमपाइमा के कारण बच्चे के फेफड़ों पर दबाव पड़ता है और तेज़ बुखार भी हो सकता है। पूर्व काल में एमपाइमा के उपचार हेतु दो पसलियों के बीच एक नली रख कर मवाद के अपनेआप सुख जाने की अथवा बाहर रीस जाने की प्रतीक्षा की जाती थी। इसके लिए बच्चे को हफ्तों और कई बार तो महीनों तक अस्पताल में भर्ती होना पड़ता था। लेकिन वर्तमान में आधुनिक उपकरणों के चलते और लेप्रोस्कोपी तकनीक के आने से दो पसलियों के बीच दूरबीन लगाकर फेफड़ों के बाहर का मवाद और प्रवाही को पूरी तरह साफ कर दिया जाता है। इस ऑपरेशन के पश्चात बच्चे को तीन से पाँच दिन अस्पताल में रहना पड़ता है जिसके बाद बच्चा सम्पूर्ण स्वस्थ हो जाता है। दूरबीन की इस टेकनीक को थोरेकोस्कोपी कहा जाता है। •